|
The term "obstetrical
palsy" was first used by Duchenne in 1872,
and the description of upper root injury was described
by Erb in 1874. The first surgical management of obstetric
brachial plexus injury
(OBPI) was reported in the early 1900's although
results were poor and mortality was present.
The majority of children with obstetric brachial
plexus injuries have risk factors for a difficult
delivery such as large size, use of forceps or vacuum,
and shoulder dystocia.
The successful surgical
treatment of brachial plexus injuries awaited
the development of microsurgical techniques in the
1970's.
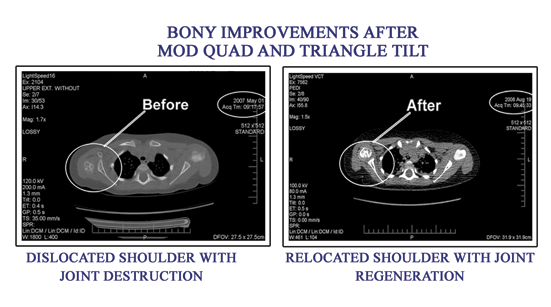
The initial treatment protocols included nerve grafting by 3 months of age. More recent studies offer the option of no nerve grafting, and instead focusing on muscle (MODIFIED QUAD) and bony (TRIANGLE TILT) surgery. In my experience, Nerve Grafting is a complicated and usually unnecessary procedure which in my research may cause worse outcomes long- term than just Muscle and Bone surgeries. Muscle and bone surgeries take less time, have less morbidity and offer significantly better outcomes than Nerve grafting alone in my experience.
|